Getting patients started
For adults with obesity (BMI of ≥30 kg/m2), or with overweight (BMI of 27 kg/m2) with at least 1 weight-related comorbidity as an adjunct to a reduced-calorie diet and increased physical activity.1
Zepbound is not for cosmetic weight loss
Here's what to do:
*For eligible and commercially insured patients on Zepbound. Governmental beneficiaries excluded, apply.
Access additional resources
- Order a demo pen kit
- Request a sales representative
By providing my professional information, I agree that it may be used by Eli Lilly and Company ("Lilly") and its affiliates and partners or third parties, working on Lilly's behalf, for Lilly's marketing or promotional purposes. I may unsubscribe/opt-out by clicking the unsubscribe link within any email I receive or by calling 1-800-LILLYRX (1-800-545-5979). For more information about Lilly's privacy practices, please view the Privacy Statement.



What's needed to begin prescribing Zepbound?
- Initiate with the 2.5-mg dose1
- After 4 weeks, increase to the 5-mg dose1
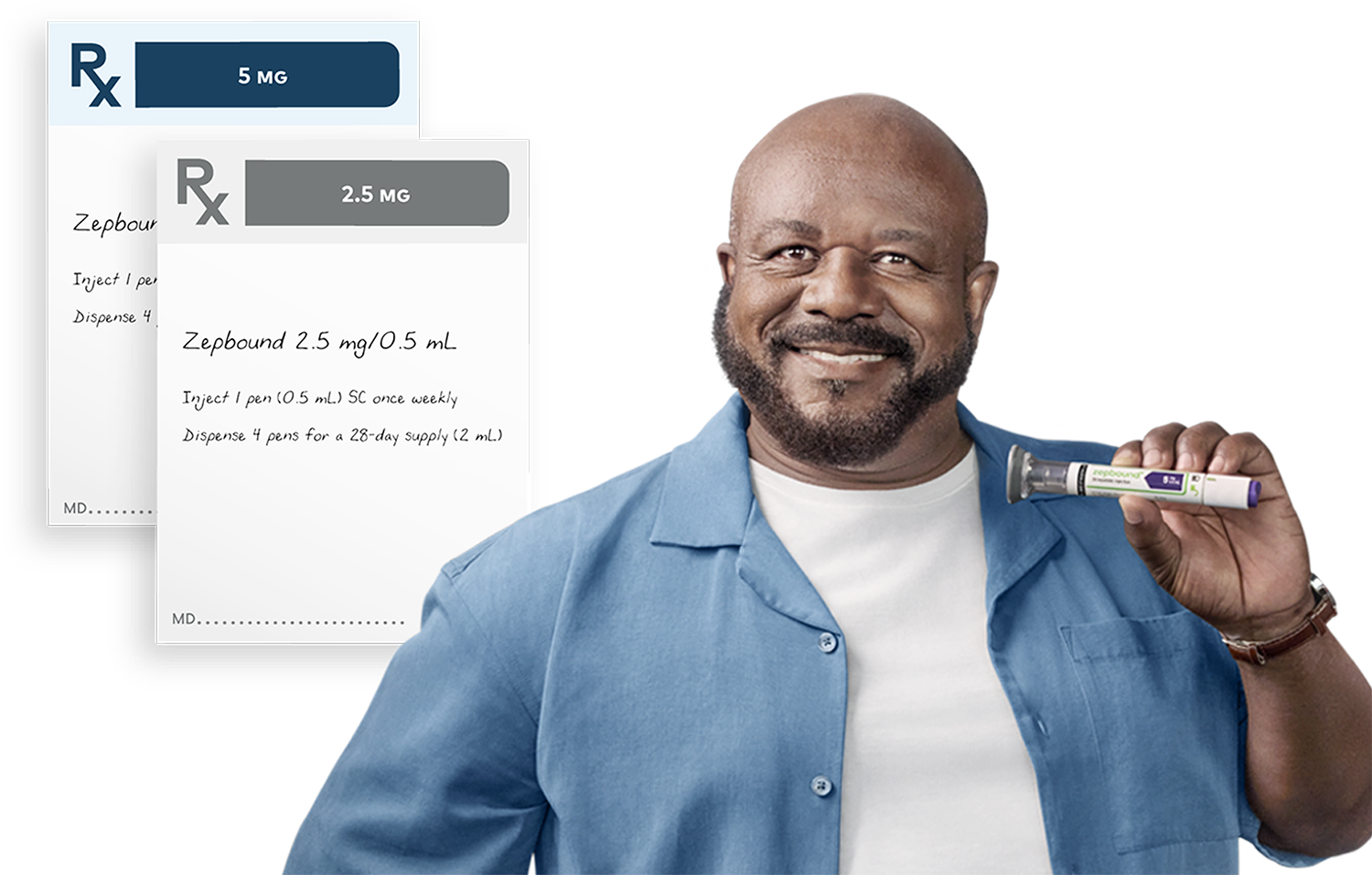
Multiple doses to help individualize treatment with Zepbound1
Recommended maintenance dosages are 5 mg, 10 mg, or 15 mg1:
You can continue to increase the dose by 2.5-mg increments after at least 4 weeks on the current dose. The maximum dose is 15 mg.1
- Consider treatment response and tolerability when selecting maintenance dosage. If not tolerated, consider a lower maintenance dosage

Image depicting the dose escalation of Zepbound. Starting dose is 2.5 mg once weekly for 4 weeks. Continue
to 5-mg maintenance dose once weekly for at least 4 weeks. The dose can be increased to 7.5 mg once weekly
for at least 4 weeks, followed by 10-mg maintenance dose once weekly for at least 4 weeks, then 12.5 mg
once
weekly for at least 4 weeks, and finally 15-mg maintenance dose once weekly as the maximum dose.
For adults with obesity (BMI of ≥30 kg/m2) or with overweight (BMI of ≥27 kg/m2) with at least 1 weight-related comorbidity as an adjunct to a reduced-calorie diet and increased physical activity.1
The 2.5-mg dosage is for treatment initiation and is not intended for chronic weight management.1
BMI=body mass index.
Relevant product information for pharmacists
Download guide
Are prior authorizations needed?
Prior authorizations are common for the incretin class. If patients' health insurance providers require prior authorizations, here's the clinical information you may need.
Requirements vary by plan. Information listed below includes common information that may be requested.


For eligible and commercially insured patients
With coverage for Zepbound

For a 1-month, 2-month, or 3-month supply if eligible and commercially insured with coverage for Zepbound

Without coverage for Zepbound

For a 1-month supply of Zepbound if eligible and commercially insured without coverage for Zepbound
aGovernmental beneficiaries excluded, terms and conditions apply.
bEstimated payment based on savings of up to $563 per month.
One month is defined as 28 days and 4 pens. Two months is defined as 56 days and 8 pens. Three months is defined as 84 days and up to 12 pens.
Access the Zepbound Savings Card for your eligible and commercially insured patients
See the savings
Send your patients to zepbound.com/coverage-savings
to explore coverage options.
Visit the site
Terms and Conditions
By enrolling in the Zepbound Savings Card Program (“Program”) and using the Zepbound Savings Card (“Card”),
you attest that you meet the eligibility criteria, and you agree to comply with the terms and conditions
described below:
Card Eligibility:
(1.) You have been prescribed Zepbound consistent with FDA approved product labeling
(2.) You are enrolled in a commercial drug insurance plan
(3.) You are not enrolled in any state, federal, or government funded healthcare program, including,
without limitation, Medicaid, Medicare, Medicare Part D, Medicare Advantage, Medigap, DoD, VA,
TRICARE®/CHAMPUS, or any state prescription drug assistance program.
(4.) You are a resident of the United States or Puerto Rico
(5.) You are 18 years of age or older
Card Terms and Conditions
For patients with commercial drug insurance coverage for Zepbound: You must have commercial drug
insurance that covers Zepbound®(tirzepatide) and a prescription consistent with FDA-approved
product
labeling to pay as little as $25 for a 1-month, 2-month, or 3-month prescription fill of Zepbound. Month is
defined as 28-days and up to 4 pens. Card savings are subject to a maximum monthly savings of up to $150 per
1-month prescription, $300 per 2-month prescription, or $450 per 3-month prescription fill and separate
maximum annual savings of up to $1,800 per calendar year. Card may be used for a maximum of up to 13
prescription fills per calendar year. Participation in the Program requires a valid patient HIPAA
authorization. Subject to Lilly USA, LLC’s (“Lilly”) right to terminate, rescind, revoke, or amend Card
eligibility criteria and/or Card terms and conditions which may occur at Lilly’s sole discretion, without
notice, and for any reason, Card expires and savings end on 12/31/2024.
For patients with commercial drug insurance who do not have coverage for Zepbound: You must have commercial drug insurance that does not cover Zepbound and a prescription consistent with FDA-approved product labeling to obtain savings of up to $563 off your 1-month prescription fill of Zepbound. Month is defined as 28-days and up to 4 pens. Card savings are subject to a maximum monthly savings of up to $563 and a separate maximum annual savings of up to $7,319 per calendar year. Card may be used for a maximum of up to 13 prescription fills per calendar year. Participation in the Program requires a valid patient HIPAA authorization. Subject to Lilly’s right to terminate, rescind, revoke, or amend Card eligibility criteria and/or Card terms and conditions which may occur at Lilly’s sole discretion, without notice, and for any reason, Card expires and savings end on 12/31/2024.
Additional Terms and Conditions
If you have an insurance plan that is participating in an alternate funding program (“AFP”) (examples
include, but are not limited to, ImpaxRX, Payer Matrix, SHARx, Script Sourcing, and Paydhealth) that
requires you to apply to the Zepbound Savings Card Program or otherwise pursue specialty drug prescription
coverage through an alternate funding vendor as a condition of, requirement for, or prerequisite to coverage
of Zepbound, you are not eligible for and are prohibited from using the Zepbound Savings Card Program. AFPs
include programs where coverage, reimbursement, or patient out of pocket costs for a product in some way
vary based on the availability of a manufacturer co-pay program. AFPs may modify, delay, deny, restrict, or
withhold insurance benefits or coverage from patients, or exclude Lilly products from coverage contingent
upon a member’s use of Zepbound Savings Card Program. You agree to inform the Zepbound Savings Card Program
if you are or become a member of such an alternative funding program. You are responsible for any applicable
taxes, fees, and any amount that exceeds the monthly or annual maximum Card savings. Monthly and annual
maximum savings are set at Lilly’s sole and absolute discretion and may be changed with or without notice at
any time for any reason. At its sole discretion and with or without notice, Lilly may reduce, eliminate, or
otherwise modify the Card savings for any reason, including but not limited to if your commercial drug
insurance plan imposes additional requirements which limits or prevents you from receiving coverage for
Zepbound, only allows partial coverage for Zepbound, removes coverage for Zepbound and requires you to
utilize the Card, does not provide a material level of financial assistance for the cost of Zepbound, or
does not apply Card payments to satisfy your co-payment, deductible, or coinsurance for Zepbound. Card
savings are not valid for: Massachusetts residents if an AB-rated generic equivalent is available;
California residents if an FDA-approved therapeutic equivalent is available. You must meet the Card
eligibility criteria, terms and conditions every time you use the Card. Card activation is required. No
party may seek reimbursement from your health insurance, any third party, or any health savings, flexible
spending, or other healthcare reimbursement accounts, for any amount of the savings received through the
Card. By utilizing the Card, you agree that if you are required to do so under the terms of your insurance
coverage for this prescription or are otherwise required to do so by law, you will notify your Insurance
Carrier of your redemption of the Card. Card savings cannot be combined or utilized with any other program,
discount, discount card, cash discount card, coupon, incentive, or similar offer involving Zepbound. You
agree that this Card savings is intended solely for the benefit of you, the patient, and that the Card
benefits are nontransferable. It is prohibited for any person to sell, purchase, or trade; or to offer to
sell, purchase, or trade, or to counterfeit the Card. The Card is not insurance. Lilly has the sole right to
interpret and apply Card eligibility criteria, and terms and conditions. Card eligibility, and terms and
conditions may be terminated, rescinded, revoked, or amended by Lilly at any time without notice and for any
reason. Eligibility criteria, and terms and conditions for the Zepbound Savings Card Program may change from
time to time; the most current version can be found at https://zepbound.lilly.com/coverage-savings. You may
be required to obtain a new Card, including if any Card terms and conditions have been terminated,
rescinded, revoked, or amended by Lilly. Card void where prohibited by law. Subject to Lilly’s right to
terminate, rescind, revoke or amend Card eligibility criteria and/or Card terms and conditions which may
occur at Lilly’s sole discretion, without notice, and for any reason, the Card expires and savings end on
12/31/2024.

REMIND Patients that Zepbound is administered using a single-dose pen. There is no need to see or handle the needle2*
ADVISE Patients to read the Instructions for Use3
ALLOW Patients to practice the injection using the demonstration device
CONSIDER having patients administer the first dose in the office
DISCUSS SAFETY profile and that Zepbound may cause some side effects†
For example, patients may experience nausea, diarrhea, or vomiting.1
In order to mitigate these gastrointestinal side effects, they may find it helpful to4-6:
- Eat smaller meals—suggest that they split 3 daily meals into 4 or more smaller meals
- Stop eating when they feel full
- Avoid fatty foods
- Try eating bland foods
Select Important Safety Information
Severe Gastrointestinal Disease: Use of Zepbound has been associated with gastrointestinal adverse reactions, sometimes severe. In clinical trials, severe gastrointestinal adverse reactions were reported more frequently among patients receiving Zepbound (5 mg 1.7%, 10 mg 2.5%, 15 mg 3.1%) than placebo (1.0%). Zepbound has not been studied in patients with severe gastrointestinal disease, including severe gastroparesis, and is therefore not recommended in these patients.
Encourage patients to continue to drink plenty of water and eat healthy meals to ensure they meet their needs for protein, micronutrients, fiber, and fluids
RECOMMEND that patients who are using oral hormonal contraceptives switch to a non-oral contraceptive method, or add a barrier method of contraception, for 4 weeks after initiation with Zepbound and for 4 weeks after each dose escalation. Zepbound delays gastric emptying, so it may make oral contraceptives less effective.1

For adult patients with obesity (BMI ≥30 kg/m2) or overweight (BMI ≥27 kg/m2) with at least 1 weight-related comorbidity as an adjunct to a reduced-calorie diet and increased physical activity.1
*If a dose is missed, instruct patients to administer Zepbound as soon as possible within 4 days after the missed dose. If more than 4 days have passed, skip the missed dose and administer the next dose on the regularly scheduled day.
†Side effects may vary and should be evaluated by the healthcare provider for appropriate management.
Watch how to use the Zepbound pen
Share this patient injection video with your patient to help them get familiar with self-injecting Zepbound.
00:00-00:05
[Animated intro sequence appears]
CAPTION: Before Janeth’s story, please see the safety information.
00:05-00:09
[Animated intro sequence with Zepbound Logo appears]
CAPTION: once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg | 15 mg
A Lilly Medicine visit www.zepbound.lilly.com or call 1-800-LillyRX for pricing information
00:09-00:52
[Opening indication appears and remains on-screen until the narrator concludes]
NARRATOR: Zepbound is an injectable prescription medicine that may help adults with obesity, or with excess weight (overweight) who also have weight-related medical problems, lose weight and keep it off. Zepbound should be used with a reduced-calorie diet and increased physical activity.
Zepbound contains tirzepatide and should not be used with other tirzepatide-containing products or any GLP-1 receptor agonist medicines. It is not known if Zepbound is safe and effective when taken with other prescription, over-the-counter, or herbal weight loss products. It is not known if Zepbound can be used in people who have had pancreatitis. It is not known if Zepbound is safe and effective for use in children under 18 years of age.
00:53-01:37
NARRATOR: Select Safety Information. Warning. Tell your healthcare provider if you get a lump or swelling in your neck, hoarseness, trouble swallowing, or shortness of breath. These may be symptoms of thyroid cancer. In studies with rats, Zepbound and medicines that work like Zepbound caused thyroid tumors, including thyroid cancer. It is not known if Zepbound will cause thyroid tumors, or a type of thyroid cancer called medullary thyroid carcinoma (MTC) in people. Do not take Zepbound if you or any of your family have ever had MTC or if you have an endocrine system condition called Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
CAPTION: See Indication and Safety Summary with Warnings at the end of this video.
01:37-01:57
[Ambient music, ocean waves, and seagull sounds play in the background; Janeth walking along the beach]
CAPTION: Janeth was a clinical trial patient and was compensated for her time.
JANETH: I tried so many things to lose weight, and I couldn't. I felt stuck in my situation.
01:57-02:17
[Ambient music continues while photos of Janeth and her family are shown]
JANETH: All my thought was food. Morning, afternoon, at night. Maybe I ate lunch, and half an hour to one hour and a half, I was hungry again. When everybody sleeping,
02:17-02:22
[Janeth speaking to the camera]
JANETH: I got hungry at one or two o'clock in the morning. I had to get up, go to the fridge
02:22-02:26
[Janeth walking along the beach]
JANETH: and get something. And when I finish from work,
02:26-02:36
[Janeth speaking to the camera]
JANETH: I pass by restaurants or fast food, and I get something for me before then I go home. When I go home, I cook, and I eat again.
02:36-02:42
[Janeth walking along the beach]
JANETH: My struggle with the weight started after having my second kid. Before I have a kid,
02:42-02:48
[Photos of Janeth and her family are shown]
JANETH: I will say I was on average size, probably six or eight. Then one day I found out myself as size 18.
02:48-02:54
[Janeth is on-screen speaking, looking at a photo of her and her sister]
JANETH: When I see this picture is, it's me and my sister on my birthday.
02:54-02:58
[Close-up of the photo of her and her sister]
It's sad to see that picture, really.
02:58-03:03
[Janeth is on-screen speaking, looking at a photo of her and her sister]
I would, I would love to erase it, but only because my sister there. I don’t like, I don't want to erase it,
03:03-03:07
[Close-up of the photo of her and her sister]
JANETH: but it's me. It was me.
03:07-03:21
[Janeth is on screen speaking to the camera; emotional]
JANETH: It's so sad. Sorry. So sad to be 30 years in your life for your weight. You’re hiding. You don't do anything. You miss so much time on your family.
03:21-03:27
[Ambient music fades out; Janeth walking into her bedroom]
JANETH: So, years passed by, and now that I'm my age,
03:27-03:29
[Janeth walks into the bedroom and opens the curtains]
JANETH: I feel like, I want to do something.
03:29-03:37
[Inspirational music plays in the background; Janeth walks into the kitchen with a grocery bag]
CAPTION: Individual results may vary. Talk to your doctor to see if Zepbound® is right for you.
JANETH: When I did the trial, it take away the desire of food.
03:37-03:44
[Janeth is putting the groceries away in her kitchen]
CAPTION: Throughout a 17-month clinical trial, people who dieted, exercised*, and took Zepbound sustained weight loss—whether taking the 5-mg, 10-mg, or 15-mg dose.†
*Reduced-calorie diet and increased physical activity.
JANETH: I was eating healthy and exercise. During 72 weeks, I was able to lose significant weight and maintain weight loss.
03:44-03:48
[Janeth on screen talking to the camera]
CAPTION: Throughout a 17-month clinical trial, people who dieted, exercised*, and took Zepbound sustained weight loss—whether taking the 5-mg, 10-mg, or 15-mg dose.†
*Reduced-calorie diet and increased physical activity.
JANETH: My size, it was, it was going low. Like size 16,
03:48-03:51
[Janeth sorts through clothes on a clothing rack]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: it went down to 14, and after that,
03:51-03:53
[Janeth picks out a coral top and holds it up against herself while looking in the mirror]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: I went down to 12, and I now it's size eight.
03:53-04:02
[Janeth washes vegetables. Janeth on screen talking to the camera]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: Before I, when I was overweight, my mind all the times think about food. Always.
04:02-04:03
[Janeth cutting vegetables]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: I look for excuse to and tell my kids,
04:04-04:08
[Janeth on screen talking to the camera]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: "You want something? You want something? Okay, I cook something for you." When I cook something for them,
04:08-04:09 [Janeth cutting vegetables]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: and for me.
04:09-04:16
[Janeth on screen talking to the camera]
JANETH: Now, really, I can cook and do everything, and it doesn't feel like I want to eat. I have the control.
04:16-04:18
[Janeth puts chopped vegetables in a bowl]
04:18-04:21
[Janeth mixes something in a saucepan]
JANETH: Since
04:21-04:22
[Janeth seasons salmon]
JANETH: losing weight,
04:23-04:24
[Janeth smiles and pours olive oil in a bowl]
JANETH: I'm more active now.
04:24-04:27
[Janeth adds seasoning to the bowl]
JANETH: Like I go to the pool, go to the park, go to the movie.
04:27-04:30
[Janeth places food on the grill]
Somebody invite me for party, like my family, I go,
04:30-04:31
[Janeth brings a plate of food over to a table]
JANETH: I go to them.
04:31-04:433
[Janeth smiling at an outdoor table during a meal]
04:33-04:34
[Janeth’s husband smiling at a table during a meal]
04:34-04:36
[Janeth and her sister take a selfie at the table]
04:36-04:38
[Janeth smiling into the camera]
JANETH: I feel happy when I see myself in the mirror.
04:38-04:42
[Janeth replaces the photo of her and her sister with a new photo]
JANETH: I am excited about where I am today
04:42-04:46
[We see the new photo Janeth has placed is the selfie with her sister taken at dinner]
JANETH: and where I want to go. I would like to
04:46-04:56
[Janeth on screen speaking to the camera]
JANETH: go back to school, finish my degree. I would like to lose more weight. I would like to have more time with my kids, my grandkids.
04:56-04:59
[Janeth puts on headphones on the beach]
JANETH: I will tell you it's a hope to lose weight.
04:59-05:07
[Janeth is power walking on the beach]
JANETH: If I did it, you can do it. I am still on my journey, and I'm not finished.
05:07-05:14
[Janeth is walking toward the camera on the beach]
JANETH: I am hopeful about where I am going.
05:14-05:19
[Janeth smiling at the camera while on the beach]
JANETH: I am unstoppable.
05:20-05:25
[Animated Zepbound logo appears on screen]
CAPTION: once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5mg | 5mg | 7.5mg | 10mg | 12.5 mg | 15mg
A Lilly Medicine visit www.zepbound.lilly.com or call 1-800-LillyRX for pricing information
05:20-05:31
[Animated Lilly Medicine logo appears on screen]
CAPTION: Lilly
A MEDICINE COMPANY
05:31-06:23
[Animated data and safety claims appear on screen]
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Indication and Safety Summary with Warnings. Zepbound® is an injectable prescription medicine that may help adults with obesity, or with excess weight (overweight) who also have weight-related medical problems, lose weight and keep it off. It should be used with a reduced-calorie diet and increased physical activity. Zepbound contains tirzepatide and should not be used with other tirzepatide-containing products or any GLP-1 receptor agonist medicines. It is not known if Zepbound is safe and effective when taken with other prescription, over-the-counter, or herbal weight loss products. It is not known if Zepbound can be used in people who have had pancreatitis. It is not known if Zepbound is safe and effective for use in children under 18 years of age.
06:23-7:40
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly zepbound® (tirzepatide) injection 0.5 mL 2.5mg | 5mg | 7.5mg | 10mg | 12.5 mg| 15mg
NARRATOR: Warnings. Zepbound may cause tumors in the thyroid, including thyroid cancer. Watch for possible symptoms, such as a lump or swelling in the neck, hoarseness, trouble swallowing, or shortness of breath. If you have any of these symptoms, tell your healthcare provider. Do not use Zepbound if you or any of your family have ever had a type of thyroid cancer called medullary thyroid carcinoma (MTC). Do not use Zepbound if you have Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Do not use Zepbound if you have had a serious allergic reaction to tirzepatide or any of the ingredients in Zepbound. Zepbound may cause serious side effects, including, severe stomach problems. Stomach problems, sometimes severe, have been reported in people who use Zepbound. Tell your healthcare provider if you have stomach problems that are severe or will not go away. Kidney problems (kidney failure). Diarrhea, nausea, and vomiting may cause a loss of fluids (dehydration), which may cause kidney problems. It is important for you to drink fluids to help reduce your chance of dehydration.
07:40-9:17
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Gallbladder problems. Gallbladder problems have happened in some people who use Zepbound. Tell your healthcare provider right away if you get symptoms of gallbladder problems, which may include pain in your upper stomach (abdomen), fever, yellowing of skin or eyes (jaundice), or clay-colored stools. Inflammation of the pancreas (pancreatitis). Stop using Zepbound and call your healthcare provider right away if you have severe pain in your stomach area (abdomen) that will not go away, with or without vomiting. You may feel the pain from your abdomen to your back. Serious allergic reactions. Stop using Zepbound and get medical help right away if you have any symptoms of a serious allergic reaction, including swelling of your face, lips, tongue or throat, problems breathing or swallowing, severe rash or itching, fainting or feeling dizzy, or very rapid heartbeat. Low blood sugar (hypoglycemia). Your risk for getting low blood sugar may be higher if you use Zepbound with medicines that can cause low blood sugar, such as a sulfonylurea or insulin. Signs and symptoms of low blood sugar may include dizziness or light-headedness, sweating, confusion or drowsiness, headache, blurred vision, slurred speech, shakiness, fast heartbeat, anxiety, irritability, mood changes, hunger, weakness or feeling jittery.
09:17-10:11
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Changes in vision in patients with type 2 diabetes. Tell your healthcare provider if you have changes in vision during treatment with Zepbound. Depression or thoughts of suicide. You should pay attention to changes in your mood, behaviors, feelings or thoughts. Call your healthcare provider right away if you have any mental changes that are new, worse, or worry you. Common side effects. The most common side effects of Zepbound include nausea, diarrhea, vomiting, constipation, stomach (abdominal) pain, indigestion, injection site reactions, feeling tired, allergic reactions, belching, hair loss, and heartburn. These are not all the possible side effects of Zepbound. Talk to your healthcare provider about any side effect that bothers you or doesn’t go away.
10:11-11:15
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Tell your healthcare provider if you have any side effects. You can report side effects at 1-800-FDA-1088 or www.fda.gov/medwatch. Before using Zepbound. Your healthcare provider should show you how to use Zepbound before you use it for the first time. Tell your healthcare provider if you are taking medicines to treat diabetes including insulin or sulfonylureas which could increase your risk of low blood sugar. Talk to your healthcare provider about low blood sugar levels and how to manage them. If you take birth control pills by mouth, talk to your healthcare provider before you use Zepbound. Birth control pills may not work as well while using Zepbound. Your healthcare provider may recommend another type of birth control for 4 weeks after you start Zepbound and for 4 weeks after each increase in your dose of Zepbound.
11:15-12:08
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Review these questions with your healthcare provider. Do you have other medical conditions, including problems with your pancreas or kidneys, or severe problems with your stomach, such as slowed emptying of your stomach (gastroparesis) or problems digesting food? Do you take diabetes medicines, such as insulin or sulfonylureas? Do you have a history of diabetic retinopathy? Do you take any other prescription medicines or over-the-counter drugs, vitamins, or herbal supplements? Are you pregnant, plan to become pregnant, breastfeeding, or plan to breastfeed? Zepbound may harm your unborn baby. Tell your healthcare provider if you become pregnant while using Zepbound. It is not known if Zepbound passes into your breast milk. You should talk with your healthcare provider about the best way to feed your baby while using Zepbound.
12:09-13:23
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Pregnancy Exposure Registry. There will be a pregnancy exposure registry for women who have taken Zepbound during pregnancy. The purpose of this registry is to collect information about the health of you and your baby. Talk to your healthcare provider about how you can take part in this registry, or you may contact Lilly at 1-800-LillyRx (1-800-545-5979). How to take. Read the Instructions for Use that come with Zepbound. Use Zepbound exactly as your healthcare provider says. Zepbound is injected under the skin (subcutaneously) of your stomach (abdomen), thigh, or upper arm. Use Zepbound 1 time each week, at any time of the day. Change (rotate) your injection site with each weekly injection. Do not use the same site for each injection. If you take too much Zepbound, call your healthcare provider, seek medical advice promptly, or contact a Poison Center expert right away at 1-800-222-1222.
13:24-14:09
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Learn more. Zepbound is a prescription medicine. For more information, call 1-800-LillyRx (1-800-545-5979) [or go to www.zepbound.lilly.com]. This summary provides basic information about Zepbound but does not include all information known about this medicine. Read the information that comes with your prescription each time your prescription is filled. This information does not take the place of talking with your healthcare provider. Be sure to talk to your healthcare provider about Zepbound and how to take it. Your healthcare provider is the best person to help you decide if Zepbound is right for you.
14:09 -14:17
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
CAPTION: ZP CON CBS 08NOV2023. Zepbound® and its delivery device base are registered trademarks owned or licensed by Eli Lilly and Company, its subsidiaries, or affiliates.
14:18-14:20
[Animated Zepbound logo appears on screen]
CAPTION: once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5mg | 5mg | 7.5mg | 10mg | 12.5 mg | 15mg
A Lilly Medicine
visit www.zepbound.lilly.com or call 1-800-LillyRX for pricing information
14:20-14:22
[Animated Lilly Medicine logo appears on screen]
CAPTION: Lilly
A MEDICINE COMPANY
[Animated intro sequence appears]
CAPTION: Before Janeth’s story, please see the safety information.
00:05-00:09
[Animated intro sequence with Zepbound Logo appears]
CAPTION: once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg | 15 mg
A Lilly Medicine visit www.zepbound.lilly.com or call 1-800-LillyRX for pricing information
00:09-00:52
[Opening indication appears and remains on-screen until the narrator concludes]
NARRATOR: Zepbound is an injectable prescription medicine that may help adults with obesity, or with excess weight (overweight) who also have weight-related medical problems, lose weight and keep it off. Zepbound should be used with a reduced-calorie diet and increased physical activity.
Zepbound contains tirzepatide and should not be used with other tirzepatide-containing products or any GLP-1 receptor agonist medicines. It is not known if Zepbound is safe and effective when taken with other prescription, over-the-counter, or herbal weight loss products. It is not known if Zepbound can be used in people who have had pancreatitis. It is not known if Zepbound is safe and effective for use in children under 18 years of age.
00:53-01:37
NARRATOR: Select Safety Information. Warning. Tell your healthcare provider if you get a lump or swelling in your neck, hoarseness, trouble swallowing, or shortness of breath. These may be symptoms of thyroid cancer. In studies with rats, Zepbound and medicines that work like Zepbound caused thyroid tumors, including thyroid cancer. It is not known if Zepbound will cause thyroid tumors, or a type of thyroid cancer called medullary thyroid carcinoma (MTC) in people. Do not take Zepbound if you or any of your family have ever had MTC or if you have an endocrine system condition called Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
CAPTION: See Indication and Safety Summary with Warnings at the end of this video.
01:37-01:57
[Ambient music, ocean waves, and seagull sounds play in the background; Janeth walking along the beach]
CAPTION: Janeth was a clinical trial patient and was compensated for her time.
JANETH: I tried so many things to lose weight, and I couldn't. I felt stuck in my situation.
01:57-02:17
[Ambient music continues while photos of Janeth and her family are shown]
JANETH: All my thought was food. Morning, afternoon, at night. Maybe I ate lunch, and half an hour to one hour and a half, I was hungry again. When everybody sleeping,
02:17-02:22
[Janeth speaking to the camera]
JANETH: I got hungry at one or two o'clock in the morning. I had to get up, go to the fridge
02:22-02:26
[Janeth walking along the beach]
JANETH: and get something. And when I finish from work,
02:26-02:36
[Janeth speaking to the camera]
JANETH: I pass by restaurants or fast food, and I get something for me before then I go home. When I go home, I cook, and I eat again.
02:36-02:42
[Janeth walking along the beach]
JANETH: My struggle with the weight started after having my second kid. Before I have a kid,
02:42-02:48
[Photos of Janeth and her family are shown]
JANETH: I will say I was on average size, probably six or eight. Then one day I found out myself as size 18.
02:48-02:54
[Janeth is on-screen speaking, looking at a photo of her and her sister]
JANETH: When I see this picture is, it's me and my sister on my birthday.
02:54-02:58
[Close-up of the photo of her and her sister]
It's sad to see that picture, really.
02:58-03:03
[Janeth is on-screen speaking, looking at a photo of her and her sister]
I would, I would love to erase it, but only because my sister there. I don’t like, I don't want to erase it,
03:03-03:07
[Close-up of the photo of her and her sister]
JANETH: but it's me. It was me.
03:07-03:21
[Janeth is on screen speaking to the camera; emotional]
JANETH: It's so sad. Sorry. So sad to be 30 years in your life for your weight. You’re hiding. You don't do anything. You miss so much time on your family.
03:21-03:27
[Ambient music fades out; Janeth walking into her bedroom]
JANETH: So, years passed by, and now that I'm my age,
03:27-03:29
[Janeth walks into the bedroom and opens the curtains]
JANETH: I feel like, I want to do something.
03:29-03:37
[Inspirational music plays in the background; Janeth walks into the kitchen with a grocery bag]
CAPTION: Individual results may vary. Talk to your doctor to see if Zepbound® is right for you.
JANETH: When I did the trial, it take away the desire of food.
03:37-03:44
[Janeth is putting the groceries away in her kitchen]
CAPTION: Throughout a 17-month clinical trial, people who dieted, exercised*, and took Zepbound sustained weight loss—whether taking the 5-mg, 10-mg, or 15-mg dose.†
*Reduced-calorie diet and increased physical activity.
JANETH: I was eating healthy and exercise. During 72 weeks, I was able to lose significant weight and maintain weight loss.
03:44-03:48
[Janeth on screen talking to the camera]
CAPTION: Throughout a 17-month clinical trial, people who dieted, exercised*, and took Zepbound sustained weight loss—whether taking the 5-mg, 10-mg, or 15-mg dose.†
*Reduced-calorie diet and increased physical activity.
JANETH: My size, it was, it was going low. Like size 16,
03:48-03:51
[Janeth sorts through clothes on a clothing rack]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: it went down to 14, and after that,
03:51-03:53
[Janeth picks out a coral top and holds it up against herself while looking in the mirror]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: I went down to 12, and I now it's size eight.
03:53-04:02
[Janeth washes vegetables. Janeth on screen talking to the camera]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: Before I, when I was overweight, my mind all the times think about food. Always.
04:02-04:03
[Janeth cutting vegetables]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: I look for excuse to and tell my kids,
04:04-04:08
[Janeth on screen talking to the camera]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: "You want something? You want something? Okay, I cook something for you." When I cook something for them,
04:08-04:09 [Janeth cutting vegetables]
CAPTION: †Individual results may vary. In a 72-week study of adults without diabetes, average weight loss was 15.0% (34 lbs) for 5 mg, 19.5% (44 lbs) for 10 mg, 20.9% (48 lbs) for 15 mg, and 3.1% (7 lbs) for placebo. In a 72-week study of adults with diabetes, average weight loss was 12.8% (28 lbs) for 10 mg, 14.7% (33 lbs) for 15 mg, and 3.2% (7 lbs) for placebo. Average starting weight was 231 lbs in adults without diabetes and 222 lbs in adults with diabetes.
JANETH: and for me.
04:09-04:16
[Janeth on screen talking to the camera]
JANETH: Now, really, I can cook and do everything, and it doesn't feel like I want to eat. I have the control.
04:16-04:18
[Janeth puts chopped vegetables in a bowl]
04:18-04:21
[Janeth mixes something in a saucepan]
JANETH: Since
04:21-04:22
[Janeth seasons salmon]
JANETH: losing weight,
04:23-04:24
[Janeth smiles and pours olive oil in a bowl]
JANETH: I'm more active now.
04:24-04:27
[Janeth adds seasoning to the bowl]
JANETH: Like I go to the pool, go to the park, go to the movie.
04:27-04:30
[Janeth places food on the grill]
Somebody invite me for party, like my family, I go,
04:30-04:31
[Janeth brings a plate of food over to a table]
JANETH: I go to them.
04:31-04:433
[Janeth smiling at an outdoor table during a meal]
04:33-04:34
[Janeth’s husband smiling at a table during a meal]
04:34-04:36
[Janeth and her sister take a selfie at the table]
04:36-04:38
[Janeth smiling into the camera]
JANETH: I feel happy when I see myself in the mirror.
04:38-04:42
[Janeth replaces the photo of her and her sister with a new photo]
JANETH: I am excited about where I am today
04:42-04:46
[We see the new photo Janeth has placed is the selfie with her sister taken at dinner]
JANETH: and where I want to go. I would like to
04:46-04:56
[Janeth on screen speaking to the camera]
JANETH: go back to school, finish my degree. I would like to lose more weight. I would like to have more time with my kids, my grandkids.
04:56-04:59
[Janeth puts on headphones on the beach]
JANETH: I will tell you it's a hope to lose weight.
04:59-05:07
[Janeth is power walking on the beach]
JANETH: If I did it, you can do it. I am still on my journey, and I'm not finished.
05:07-05:14
[Janeth is walking toward the camera on the beach]
JANETH: I am hopeful about where I am going.
05:14-05:19
[Janeth smiling at the camera while on the beach]
JANETH: I am unstoppable.
05:20-05:25
[Animated Zepbound logo appears on screen]
CAPTION: once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5mg | 5mg | 7.5mg | 10mg | 12.5 mg | 15mg
A Lilly Medicine visit www.zepbound.lilly.com or call 1-800-LillyRX for pricing information
05:20-05:31
[Animated Lilly Medicine logo appears on screen]
CAPTION: Lilly
A MEDICINE COMPANY
05:31-06:23
[Animated data and safety claims appear on screen]
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Indication and Safety Summary with Warnings. Zepbound® is an injectable prescription medicine that may help adults with obesity, or with excess weight (overweight) who also have weight-related medical problems, lose weight and keep it off. It should be used with a reduced-calorie diet and increased physical activity. Zepbound contains tirzepatide and should not be used with other tirzepatide-containing products or any GLP-1 receptor agonist medicines. It is not known if Zepbound is safe and effective when taken with other prescription, over-the-counter, or herbal weight loss products. It is not known if Zepbound can be used in people who have had pancreatitis. It is not known if Zepbound is safe and effective for use in children under 18 years of age.
06:23-7:40
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly zepbound® (tirzepatide) injection 0.5 mL 2.5mg | 5mg | 7.5mg | 10mg | 12.5 mg| 15mg
NARRATOR: Warnings. Zepbound may cause tumors in the thyroid, including thyroid cancer. Watch for possible symptoms, such as a lump or swelling in the neck, hoarseness, trouble swallowing, or shortness of breath. If you have any of these symptoms, tell your healthcare provider. Do not use Zepbound if you or any of your family have ever had a type of thyroid cancer called medullary thyroid carcinoma (MTC). Do not use Zepbound if you have Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Do not use Zepbound if you have had a serious allergic reaction to tirzepatide or any of the ingredients in Zepbound. Zepbound may cause serious side effects, including, severe stomach problems. Stomach problems, sometimes severe, have been reported in people who use Zepbound. Tell your healthcare provider if you have stomach problems that are severe or will not go away. Kidney problems (kidney failure). Diarrhea, nausea, and vomiting may cause a loss of fluids (dehydration), which may cause kidney problems. It is important for you to drink fluids to help reduce your chance of dehydration.
07:40-9:17
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Gallbladder problems. Gallbladder problems have happened in some people who use Zepbound. Tell your healthcare provider right away if you get symptoms of gallbladder problems, which may include pain in your upper stomach (abdomen), fever, yellowing of skin or eyes (jaundice), or clay-colored stools. Inflammation of the pancreas (pancreatitis). Stop using Zepbound and call your healthcare provider right away if you have severe pain in your stomach area (abdomen) that will not go away, with or without vomiting. You may feel the pain from your abdomen to your back. Serious allergic reactions. Stop using Zepbound and get medical help right away if you have any symptoms of a serious allergic reaction, including swelling of your face, lips, tongue or throat, problems breathing or swallowing, severe rash or itching, fainting or feeling dizzy, or very rapid heartbeat. Low blood sugar (hypoglycemia). Your risk for getting low blood sugar may be higher if you use Zepbound with medicines that can cause low blood sugar, such as a sulfonylurea or insulin. Signs and symptoms of low blood sugar may include dizziness or light-headedness, sweating, confusion or drowsiness, headache, blurred vision, slurred speech, shakiness, fast heartbeat, anxiety, irritability, mood changes, hunger, weakness or feeling jittery.
09:17-10:11
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Changes in vision in patients with type 2 diabetes. Tell your healthcare provider if you have changes in vision during treatment with Zepbound. Depression or thoughts of suicide. You should pay attention to changes in your mood, behaviors, feelings or thoughts. Call your healthcare provider right away if you have any mental changes that are new, worse, or worry you. Common side effects. The most common side effects of Zepbound include nausea, diarrhea, vomiting, constipation, stomach (abdominal) pain, indigestion, injection site reactions, feeling tired, allergic reactions, belching, hair loss, and heartburn. These are not all the possible side effects of Zepbound. Talk to your healthcare provider about any side effect that bothers you or doesn’t go away.
10:11-11:15
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Tell your healthcare provider if you have any side effects. You can report side effects at 1-800-FDA-1088 or www.fda.gov/medwatch. Before using Zepbound. Your healthcare provider should show you how to use Zepbound before you use it for the first time. Tell your healthcare provider if you are taking medicines to treat diabetes including insulin or sulfonylureas which could increase your risk of low blood sugar. Talk to your healthcare provider about low blood sugar levels and how to manage them. If you take birth control pills by mouth, talk to your healthcare provider before you use Zepbound. Birth control pills may not work as well while using Zepbound. Your healthcare provider may recommend another type of birth control for 4 weeks after you start Zepbound and for 4 weeks after each increase in your dose of Zepbound.
11:15-12:08
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Review these questions with your healthcare provider. Do you have other medical conditions, including problems with your pancreas or kidneys, or severe problems with your stomach, such as slowed emptying of your stomach (gastroparesis) or problems digesting food? Do you take diabetes medicines, such as insulin or sulfonylureas? Do you have a history of diabetic retinopathy? Do you take any other prescription medicines or over-the-counter drugs, vitamins, or herbal supplements? Are you pregnant, plan to become pregnant, breastfeeding, or plan to breastfeed? Zepbound may harm your unborn baby. Tell your healthcare provider if you become pregnant while using Zepbound. It is not known if Zepbound passes into your breast milk. You should talk with your healthcare provider about the best way to feed your baby while using Zepbound.
12:09-13:23
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Pregnancy Exposure Registry. There will be a pregnancy exposure registry for women who have taken Zepbound during pregnancy. The purpose of this registry is to collect information about the health of you and your baby. Talk to your healthcare provider about how you can take part in this registry, or you may contact Lilly at 1-800-LillyRx (1-800-545-5979). How to take. Read the Instructions for Use that come with Zepbound. Use Zepbound exactly as your healthcare provider says. Zepbound is injected under the skin (subcutaneously) of your stomach (abdomen), thigh, or upper arm. Use Zepbound 1 time each week, at any time of the day. Change (rotate) your injection site with each weekly injection. Do not use the same site for each injection. If you take too much Zepbound, call your healthcare provider, seek medical advice promptly, or contact a Poison Center expert right away at 1-800-222-1222.
13:24-14:09
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
NARRATOR: Learn more. Zepbound is a prescription medicine. For more information, call 1-800-LillyRx (1-800-545-5979) [or go to www.zepbound.lilly.com]. This summary provides basic information about Zepbound but does not include all information known about this medicine. Read the information that comes with your prescription each time your prescription is filled. This information does not take the place of talking with your healthcare provider. Be sure to talk to your healthcare provider about Zepbound and how to take it. Your healthcare provider is the best person to help you decide if Zepbound is right for you.
14:09 -14:17
CAPTION: INDICATION AND SAFETY SUMMARY WITH WARNINGS
once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5 mg | 5 mg | 7.5 mg | 10 mg | 12.5 mg| 15 mg
CAPTION: ZP CON CBS 08NOV2023. Zepbound® and its delivery device base are registered trademarks owned or licensed by Eli Lilly and Company, its subsidiaries, or affiliates.
14:18-14:20
[Animated Zepbound logo appears on screen]
CAPTION: once weekly Zepbound® (tirzepatide) injection 0.5 mL 2.5mg | 5mg | 7.5mg | 10mg | 12.5 mg | 15mg
A Lilly Medicine
visit www.zepbound.lilly.com or call 1-800-LillyRX for pricing information
14:20-14:22
[Animated Lilly Medicine logo appears on screen]
CAPTION: Lilly
A MEDICINE COMPANY
References
- Zepbound. Prescribing Information. Lilly USA, LLC.
- Zepbound. Instructions for Use. Lilly USA, LLC.
- Zepbound. Medication Guide. Lilly USA, LLC.
- Maceira E, Lesar TS, Smith H. Medication related nausea and vomiting in palliative medicine. Ann Palliat Med. 2012;1(2):161-176.
- Kruger DF, Bode B, Spollett GR. Understanding GLP-1 analogs and enhancing patients success. Diabetes Educ. 2010;36(suppl 3):44S-72S.
- Reid TS. Practical use of glucagon-like peptide-1 receptor agonist therapy in primary care. Clin Diabetes. 2013;31(4):148-157.